Temporary mechanical circulatory support (tMCS) devices are critical tools in managing patients with severe hemodynamic instability, often employed as bridges to recovery or more permanent solutions like heart transplantation. Among the expanding array of tMCS technologies, the PulseCath system—which includes iVAC2L and iVAC3L—emerges as a promising intermediate solution. This research protocol proposes a comprehensive scoping review of both clinical and preclinical evidence supporting PulseCath, providing vital insights into its utility, advantages, and limitations.
PulseCath is a novel percutaneous left ventricular assist device (LVAD) that functions through a unique pulsatile mechanism, offering bidirectional flow via a valved catheter connected to an extracorporeal membrane pump. Its ease of use, compatibility with existing intra-aortic balloon pump (IABP) consoles, and intermediate flow rate of 2–3 L/min position it strategically between the widely-used IABP (0.5–1 L/min) and the more invasive Impella system (up to 5.5 L/min). This compatibility minimizes equipment needs and could significantly reduce the overall cost of care while expanding access in resource-limited settings.
This review protocol outlines a structured methodology rooted in the Joanna Briggs Institute (JBI) framework and PRISMA-P guidelines. The review aims to cover both in vivo preclinical trials and clinical investigations, capturing data from global sources including PubMed, EMBASE, Cochrane, Web of Science, Scopus, and Google Scholar, with a search cutoff of February 28, 2025.
The review will classify studies into two main categories: preclinical in vivo studies and clinical trials. Clinical data will be further sorted based on the implantation approach—whether pre-emptive (used before a high-risk procedure) or bail-out (used reactively during acute cardiac events). This dual-pronged categorization ensures a detailed understanding of the device’s functional and therapeutic scope across multiple patient scenarios.
One of the key strengths of PulseCath is its potential to bridge the gap between low- and high-flow support devices. While IABP is low-cost and safe but limited in efficacy, and Impella provides strong support but at the expense of greater complication risks and cost, PulseCath offers a middle ground. It can facilitate high-risk procedures such as complex percutaneous coronary interventions (PCI) and provide crucial support in cardiogenic shock, possibly with fewer vascular complications and lower incidences of hemolysis and acute kidney injury compared to Impella.
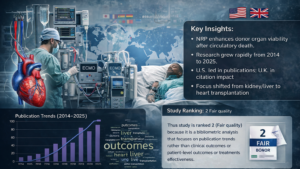
To evaluate these claims, the authors plan a rigorous review using tools like EndNote X9 and Rayyan for study selection, along with risk-of-bias assessments using ROBINS-I and RoB2 tools. The final output will feature both qualitative narrative syntheses and quantitative data, when homogeneity allows. Data tables and illustrative figures will aid in visualizing the findings.
The review will extract and chart data covering hemodynamic performance, procedural details, safety outcomes, echocardiographic changes, and interactions with other tMCS systems. This will help delineate scenarios where PulseCath performs optimally—whether as standalone therapy or as part of a hybrid support strategy.
Furthermore, the review will identify knowledge gaps and guide future clinical trials. Current literature on PulseCath remains limited and scattered, making this scoping review timely and essential for informing both clinical decisions and research priorities. The ultimate goal is to improve patient outcomes by clarifying the most effective, safe, and practical uses of this novel device.
In conclusion, the planned scoping review holds potential to significantly shape the landscape of mechanical circulatory support. By compiling a comprehensive assessment of PulseCath’s pathophysiological basis, hemodynamic impacts, and clinical applications, the review aims to enhance adoption strategies, improve care delivery, and foster future innovations in cardiovascular critical care.